Different ways to win the „battle“ against Covid-19 or:
The world wide greatest bluff
Useless:
– respiratory transmission is dominant, with proximity and ventilation being key determinants of transmission risk (Annals of Internal Medicine, 17/09/2020)
Kills the nature:
-“the bees will die and then the humans” (Einstein)
-Masks oblige people to infect themselves more and more (as if one smoked under the mask), condemning them to an increasingly serious risk to their health and producing severely ill patients.
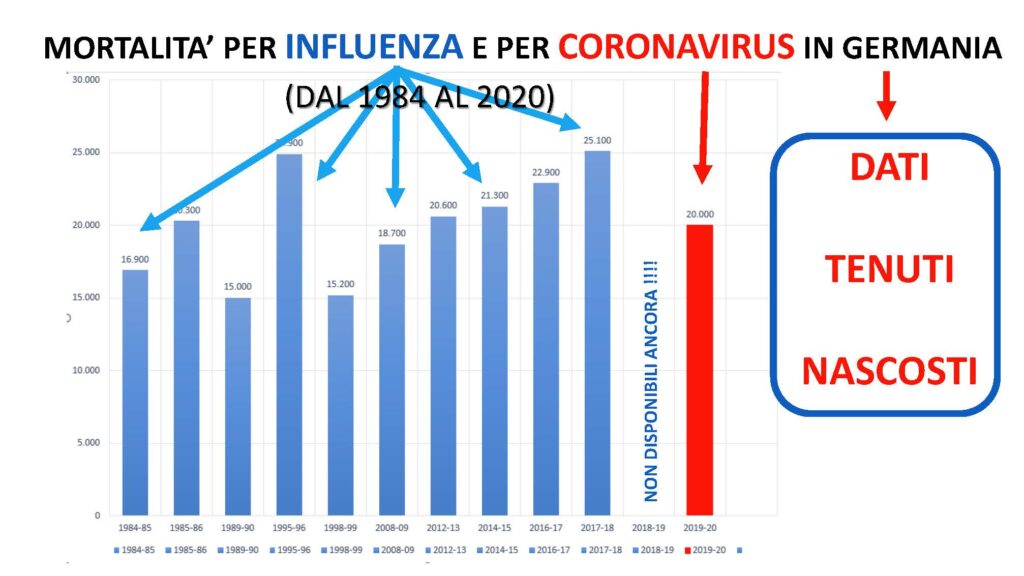
– The EU (to name some countries) spent about 1.3 billion in England, over 700 million in France and 239 million in Germany for the vaccine for the swine flu, which in the end had caused only 2900 deaths in all Europe compared to the European average for common influenza of 40.000 to 220.000 yearly (EC debate on 7/3/2011).
Dangerous:
– A 7-fold elevated risk of onset of narcolepsy after Pandemrix was found, which was confined to the first year after vaccination, with the highest risk within 6 months. (Stowe, Andrews et al., 14/09/2020)
– People with a history of significant allergic reactions should not have the Pfizer/BioNTech Covid jab, regulators say. (BBC 9/12/2020)
– The Medicines and Healthcare Products Regulatory Agency (MHRA) declares, that persons with allergic reactions (byImmunoglobuline E) should not been vaccinated (Reuters,20/12/20)
But politics and the media can falsify everything on the world.
For a livable future we need to save the micro and macro-environment and not the interests of the pharmaceutical companies and other dark powers.
Globaly, people, policies and procurement are being corrupted by political and commercial agendas. The medical-political complex tends towards suppression of science to aggrandise and enrich those in power.
– La paura dal coronavirus (Coronafobia) ha creato innumerevoli manifestazioni psichiatriche attraverso tutte le classi sociali. L’impatto della quarantena passa dai effetti immediati quali: irritabilità, paura di contrarre e trasmettere l’infezione, frustrazione, ansia, depressione, paura della solitudine, insonnia, disperazione, fino agli estremi includendo il suicidio. (Elsevier Public Health Emergency Collection, 27/05/2020).
-Le mascherine obbligano, respiro per respiro, le persone infette di ispirare i propri virus, aumentando la carica virale fino a condannarle eventualmente alla morte (Vaso di Pandora, 17/08/2020).
Uccidono l’uomo:
– Nei pazienti ventilati c’è stata una aumentata mortalità, mentre nei altri gruppi è paragonabile ad un placebo. (WHO Solidarity Consortium, 15/10/2020)
– Nel caso dell’influenza suina sono stati spesi dall’Unione Europea più di 5 Miliardi per il vaccino per una influenza, che aveva causato in Europa solo 2900 decessi rispetto alla mediaeuropea di 40.000 a 220.000 l’anno (Dibattito Comunione Europea del 7/3/2011). Gran parte del vaccino è stata poi distrutta (in Germania l’85%)
Pericolosi:
– Il vaccino contro l’influenza suina èra associata ad un notevole aumento della narcolepsia in giovani (Stowe, Andrews et al., 14/09/2020)
– Grave reazione al vaccino della Pfitzer in America (New York Times, 15/12/2020)
– La Medicines and Healthcare Products Regulatory Agency (MHRA) in Inghilterra dispone dopo le reazioni allergiche al vaccino, che persone con allergiche significative non possono essere vaccinati (Reuters,20/12/20)
– Il 48,6 % della popolazione tedesca presenta gli anticorpi E, responsabili di reazioni allergiche significative(Robert Koch Institut, 2016) ;
Avete capito, che tutto è solo un gioco di soldi, la salute non centra.
Vi chiedo un minuto di attenzione per farVi vedere, che tutto è solo un bluff gigantesco.
Per un futuro vivibile importa salvare il micro e macroambiente e non gli incassi delle dite farmaceutiche o di altri poteri occulti.
Globaly, people, policies and procurement are being corrupted by political and commercial agendas. The medical-political complex tends towards suppression of science to aggrandise and enrich those in power.
The obligation for masks is considered one of the most effective measures to combat the coronavirus pandemic. This measure is imposed, like many others, only for populist political reasons and is not only completely ineffective with regard to a reduction in the transmission of the virus, but also constitutes a serious danger to the health of anyone wearing the mask (1) (European Centre for Disease Prevention and Control 2020). This problem is sidetracked, deliberately creating great confusion among the sick, the dead, the HIV-positive, the healthy carriers, the asymptomatic, the positive etc.
In the end the contagiousness index was introduced (Robert Koch Institute) as the supreme judge of good and evil, which arbitrarily divides countries into zones of good and bad citizens, the latter to be ruthlessly punished. All this happens with no scientific basis and is statistically unacceptable, but the hunt for positives with all available means (immune App etc.) has become one of the “main weapons in the fight against the Coronavirus”. Those discovered positive and their families are put under house arrest and pilloried, as if they were criminals.
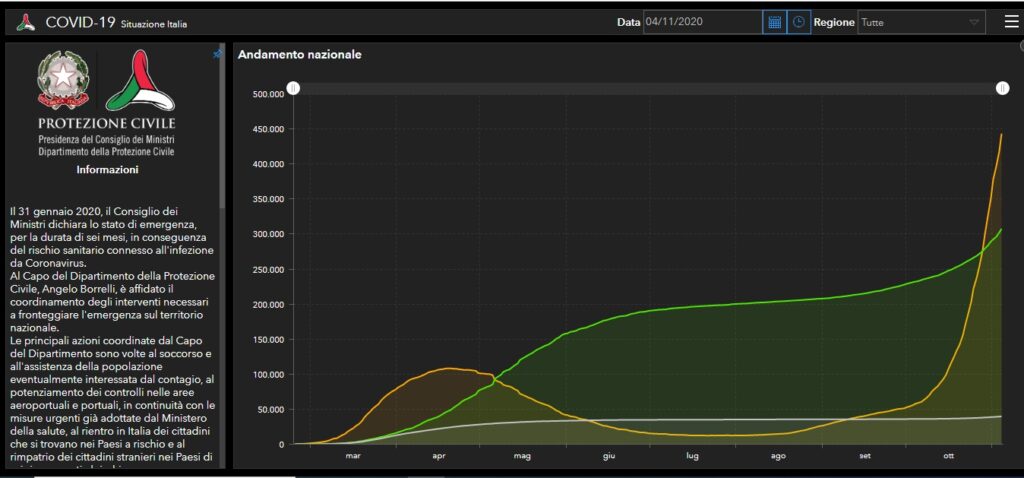
But this hunt makes no sense, as the contagiousness index is completely unrelated to mortality, as shown by the statistics issued by the Italian Ministry of Health/ Ministero della Salute Italiano on 4/11/20 (2).
Curve – yellow: currently positive, green: recovered, grey: deaths
BUT WHAT IS WRONG WITH MASKS?
I’ll explain it in a nutshell.
Our body has four elimination pathways for noxious substances: urinary tract (urine), digestive tract (feces), skin (perspiration) and the lungs (respiration). This last pathway, important with regard to coronavirus transmission, must guarantee both the oxygen/carbon dioxide exchange and the ventilation of the respiratory tracts, the nasal and paranasal sinuses and the middle ear.
If this or any other pathway is interrupted or reduced, the body gets progressively intoxicated and damaged even irreversibly.
And now we come to masks:
Masks in no way protect against coronavirus infection as the means of transmission is exclusively aerial by aerosols (3) and not through droplets or contact.
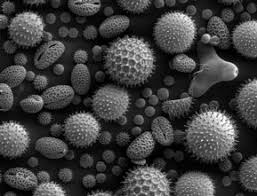
The Coronaviruses have a superimposable shape to that of various pollens (one of nature’s wonders) but they are much smaller and are transmitted in the same way, suspended and transported by air. If they land on fertile ground (for the coronavirus the peripheral airways, i.e. the bronchioles) they take root and then multiply.
CoronavirusPollen from a peanut bush
Their dimensions are also comparable to those of smoke particles, they get to the alveoli and are then inhaled and exhaled. This is the difference to droplet particles, which having a diameter about 60 times higher, are picked up by the upper respiratory tracts.
The Coronavirus’ gateway to the body and its replication finally take place at the level of the peripheral airways (bronchioles), where they induce an inflammatory response mediated by antibodies similar to allergic asthma. This is why the severity of the disease does not primarily depend on the damage caused to the organism by the virus, but on the damage caused by the immune system to the organism (4), which is why cortisone was the first choice drug in aggravated cases at the beginning of the pandemic.
The modes of falling ill with coronavirus are comparable to those of falling ill from passive smoking. Coming into contact with people who transmit coronavirus is the same as coming into contact with smokers. The harmful agent is inhaled in the same way and the dangerous load for the organism only takes place in closed, badly ventilated environments.
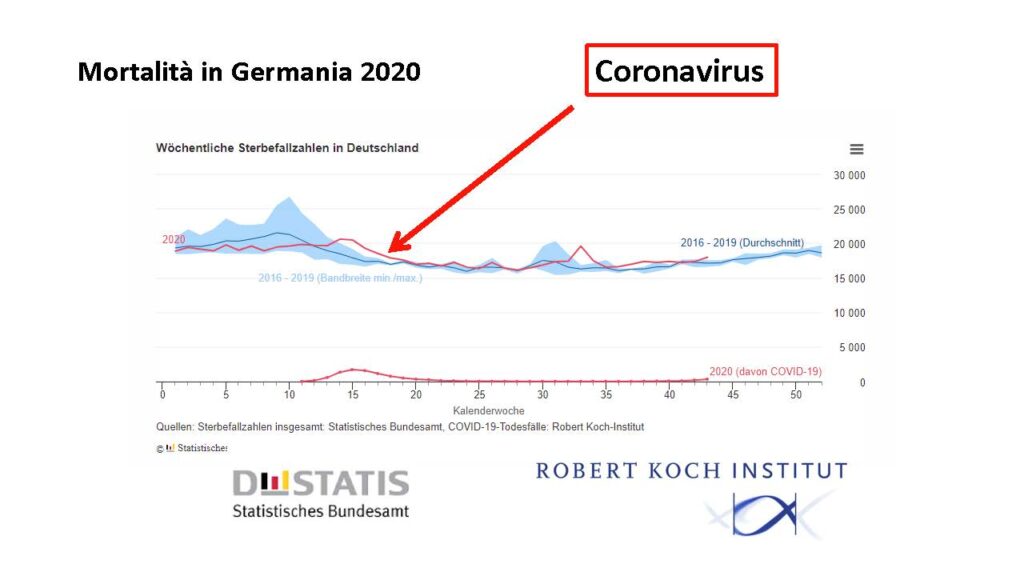
In this respect the Robert Koch Institute has confirmed that transmission of the virus in the open is highly improbable (RKI).
Masks are very dangerous because they greatly reduce the aeration of the lungs.
Once respiratory system patients were sent to the mountains or the sea to exhale the unhealthy air and inhale clean air, whereas now they are provided with masks and the exhaled air (which contains a high number of viruses during the infectious phase) cannot disperse in the open air but is retained by the mask and subsequently inhaled.
“Put on your costume”
In this respect masks oblige people to infect themselves more and more (as if one smoked under the mask), condemning them to an increasingly serious risk to their health and producing severely ill patients.
And so, breath by breath, people reduce their chances of survival. HOORAY FOR MEDICINE!
Unfortunately medicine is not a science, but an opinion. Day by day many opinions (political, economic, populist etc.) interfere on the orientation of medicine, also with compliant experts in the medical sphere. In arithmetic, (which is a science) one and one makes two (1+1=2), in medicine (which is an opinion) 1+1 does not always make 2, it eventually makes 3, 4 or 18, 24, maybe better 42-2, according to the current opinion.
With the current government measures we are actually forced to take refuge in closed places, right where we get infected and then we are forced to endure serious or very serious harm caused by the obligation for masks. We are taken right there, young and old, where we don’t want to end up, in the arms of the angel of death.
APPENDIX:
Ceterum censeo, Cartaginem esse delendam, thus Cato, the Censor finished each of his speeches at the Senate.
In this sense this contribution ends with:Ceterum Censeo, that the situation is not of a medical but a political/economic nature, public good and health have nothing to do with it, common people are nothing but cannon fodder:
Because there is a daily organized disinformation of the population regarding mortality, lethality, contagiousness index, deceased, newly infected, re-infection, asymptomatic, healthy carriers, positives. The latter are pursued with all the means at the disposal of the state, as if they were criminals. But this hunt makes no sense, as the contagiousness index is completely unrelated to mortality, as shown by the statistics issued by the Italian government on 4/11/20 (A).
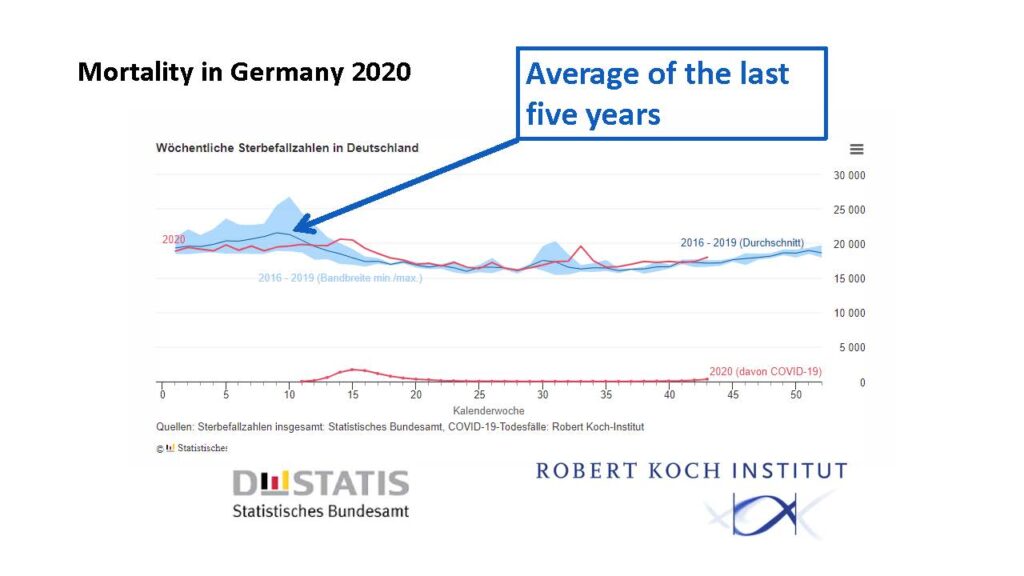
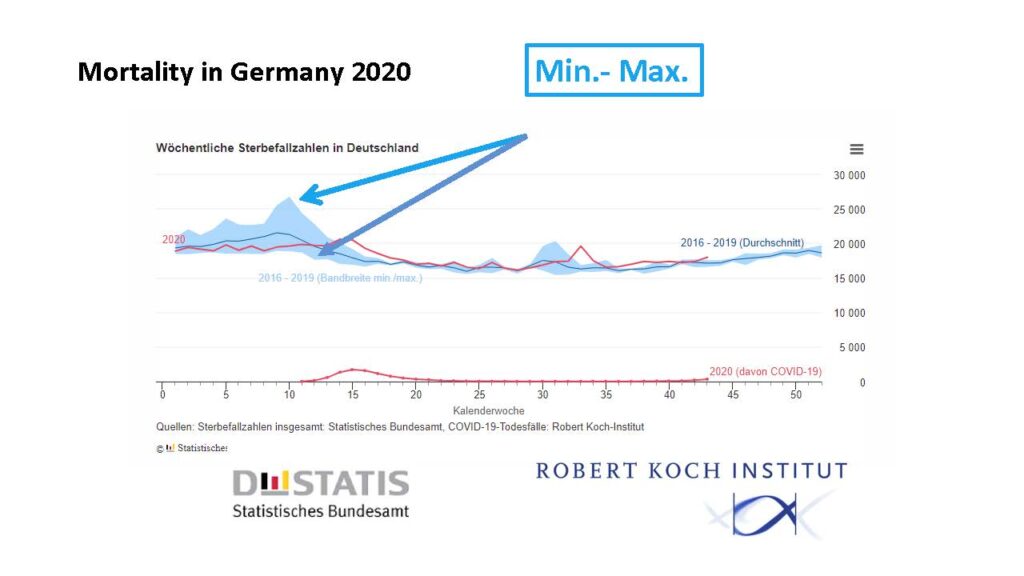
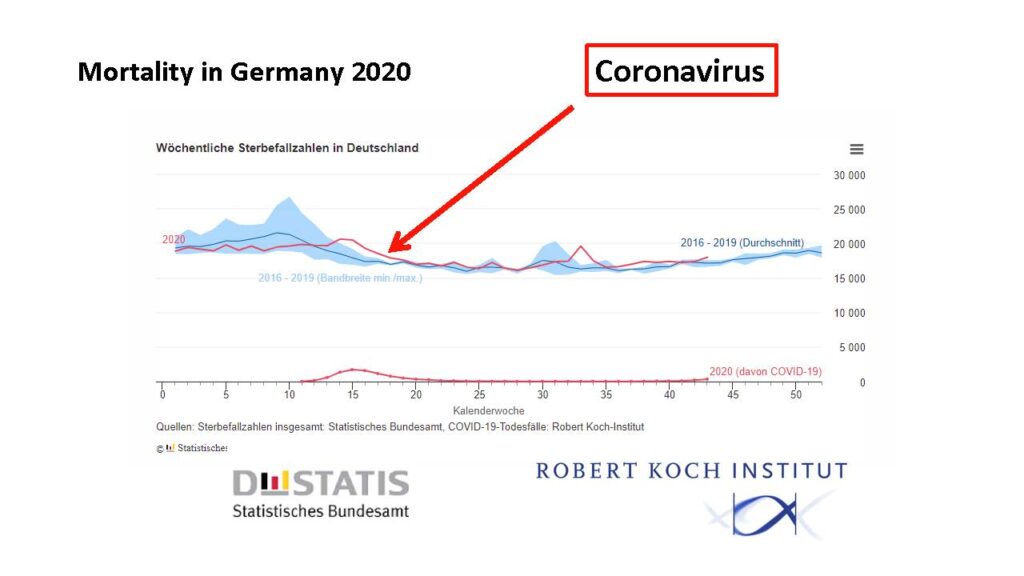
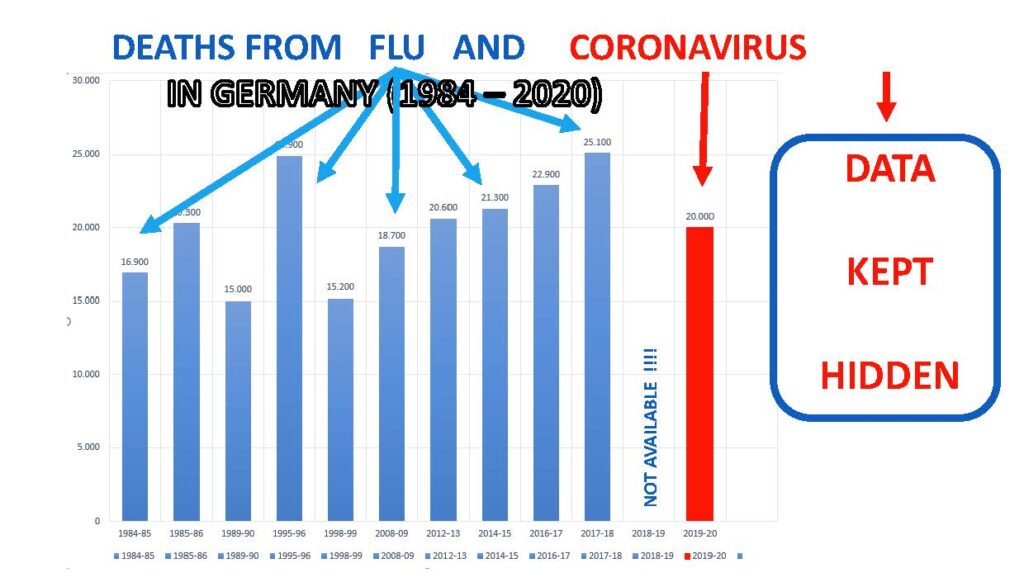
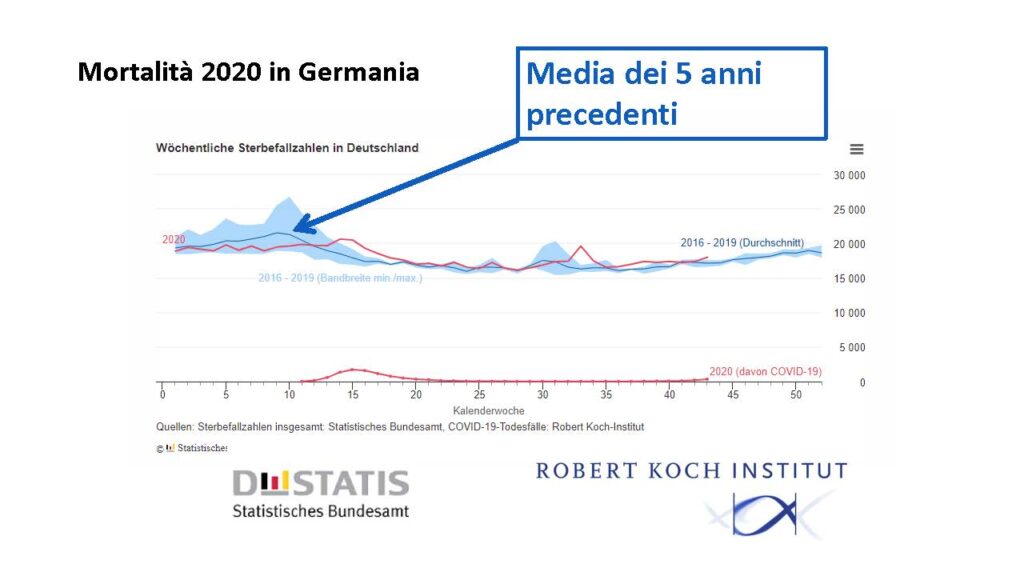
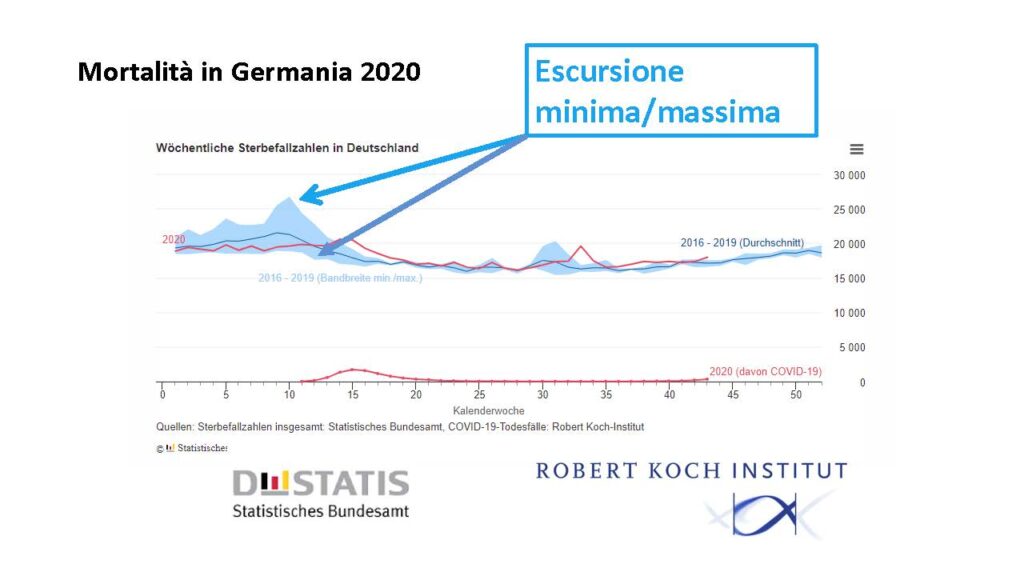
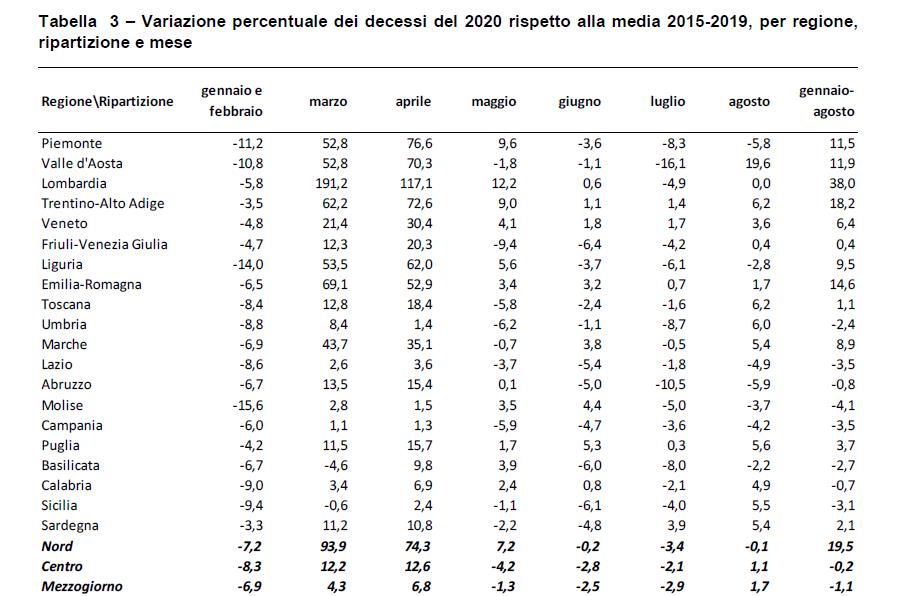
Because disastrous news is broadcast every day regarding the pandemic, even though this year (e.g. in Italy, in Germany the relevant data is not available) there has not been a statistically significant rise in mortality compared to the period 2015-2019. From May-August there was even a reduction in mortality compared to the five previous years by 1.6% (ISTAT Report, National Institute of Statistics 22/10/2020 (Table 1)(B).
Because the statistics released by the media predict a significant increase in deaths from coronavirus with distressing forecasts for the future, (“soon over 1,000 deaths a day”), even though the lethality of Coronavirus is estimated at 0.14% against the 0.10 of common ‘flu (WHO 14/10/20)(C). Possibly because even patients without laboratory confirmation are included in the deaths with only a suspected diagnosis (as a result of medical or epidemiological evaluation) (Report of the National Health Insitute (ISS), n.49/2020,8/6/20, note 1)(D), or because the statistical elaboration was carried out on limited groups of patients (4942 of 31.573 deaths from Coronavirus to 25/05/2020), or because inappropriate terms of definition were used. The term “directly responsible for death”, means that the death would not have beenverified if the SARS-CoV-2 infection had not intervened, although often overlapping other pre-existing conditions, and their complications. (Report from the “National Institute of Statistics on16/7/2020: Impact of the Covid-19 epidemic on mortality: Causes of death of SARS-CoV-2 positives, note 2)(E).
At the moment almost all the hospitals in almost all Europe are nearly full of Coronavirus patients, even though current mortality is much lower than in the spring. Also the capacity of hospital beds for coronavirus patients has increased since then. This could serve to recover the deficit of hospitals caused by the dramatic reduction in hospital admissions due to the pandemic (the deficit in the first 4 months in Italy is 3.5 bilions of Euro: Report ALTEMS) (F). In this way the Budget can be met, so as not to remain insolvent. (“Coronavirus rettet die Kliniken, aber die Pleitegefahr bleibt hoch” = the coronavirus crisis saves the hospitals, but the risk of bankruptcy remains high. Das Handelsblatt ) (G). In Germany the state pays the hospitals about 700 euro for every unoccupied bed, to keep it free for the eventual second wave of the pandemic. All this because direct subsidies at EU level are no longer permitted. If someone cannot uphold their financial obligations, they have to declare insolvency, a disaster for public healthcare.
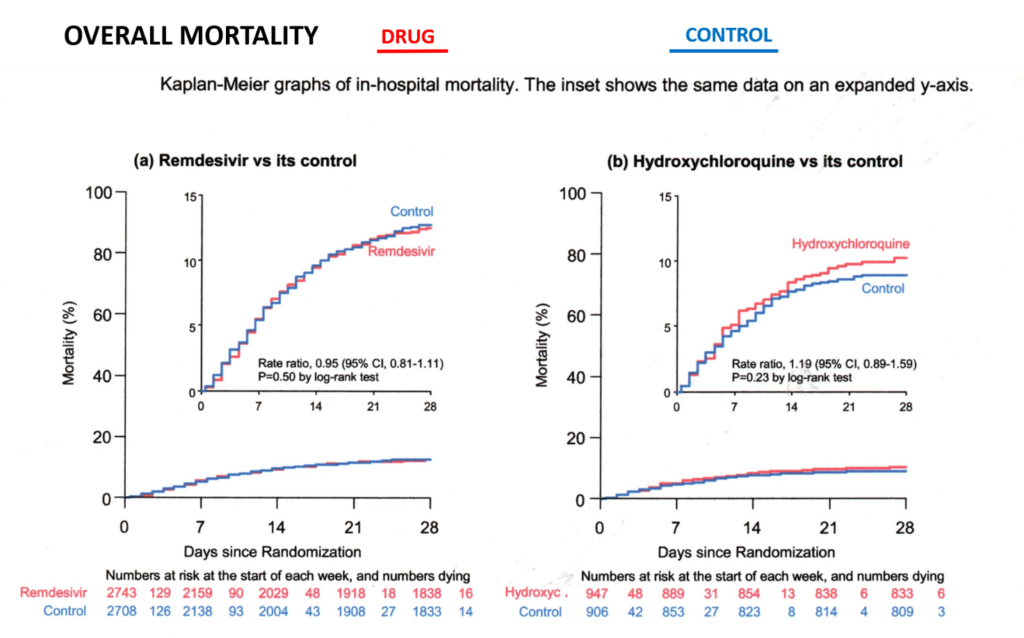
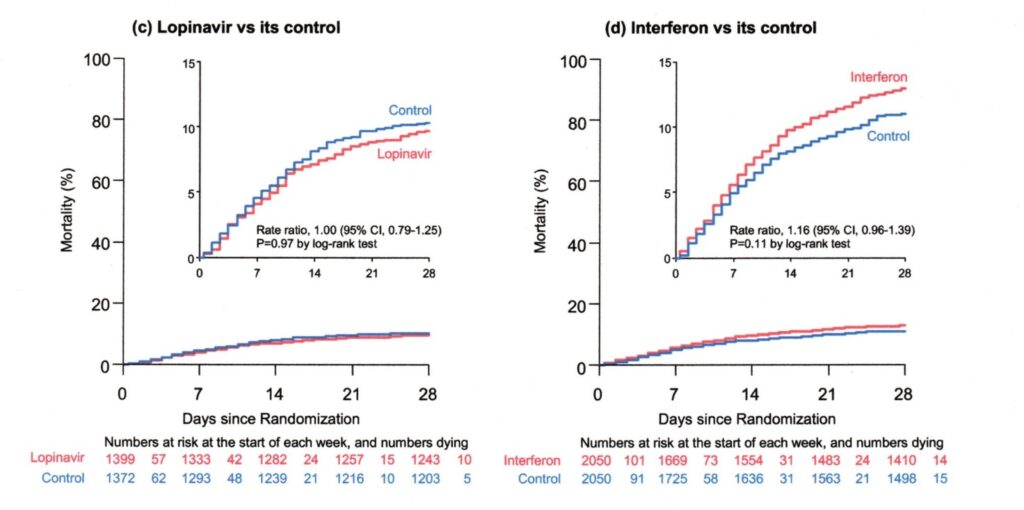
Because in March wide-spectrum trials of antiviral drugs like Remdesivir (Solodarity etc.) were authorized globally, where the control group did not receive any specific pharmacological drug, which actually should have been cortisone. In their wake the same useless medicines have been tested almost everywhere.
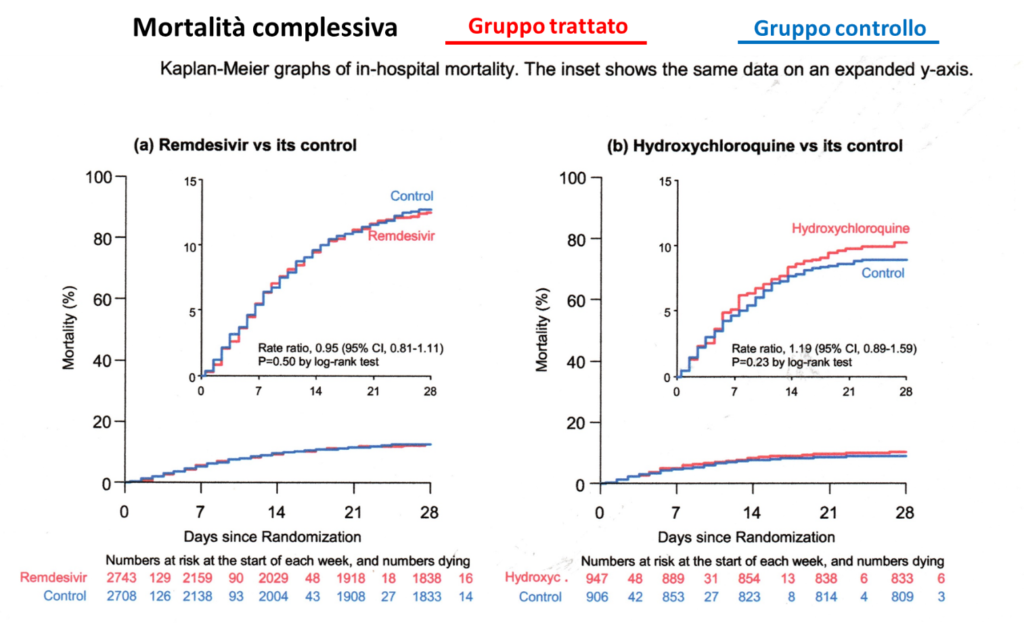
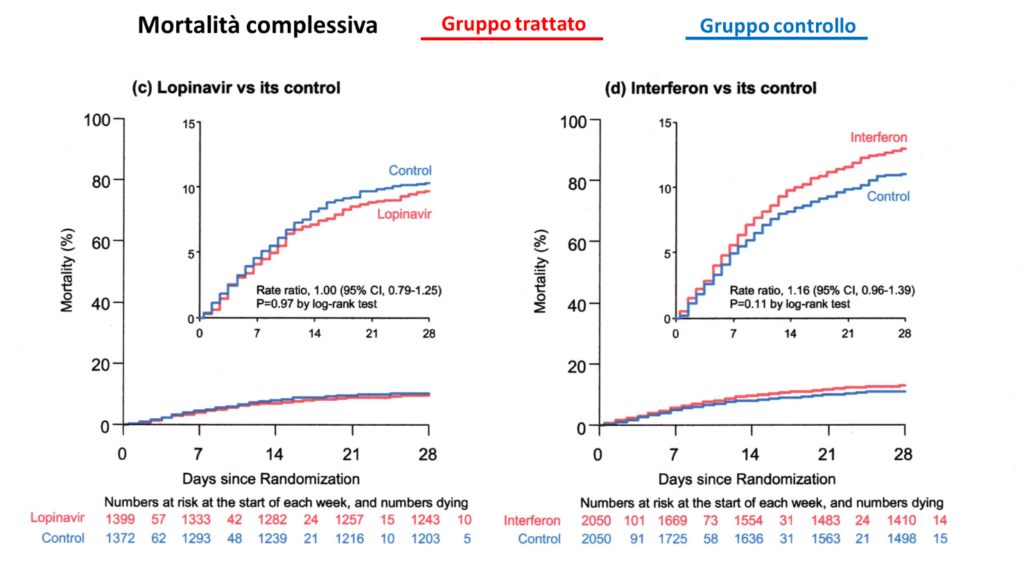
Because they insisted on testing for many months to ascertain whether the therapy was beneficial, which was already evident after a month (statistical elaboration through the Kaplan Meier 28 Day Mortality method, Table 2) (H). In fact mortality was superior to the control group. In these trials mortality for ventilated patients was 41% (Solidarity study), while with the cortisone therapy it was 29% (Recovery Study) (I).All these useless pharmaceutical trials have caused the death of thousands of people under the pretext of scientific research. And all this in general without having requested and obtained the informed consent from the patients/relatives, because a European legal provision exonerated the experimenter from this obligation for the Covid emergency (European Medicines Agency etc.) (J), seriously infringing the fundamental constitutional rights of every citizen. No patient or relative would have signed an informed consent stating that half the patients were left with no treatment but only the placebo.
Because the European governments were advised to authorize the use of Remdesivir on 3 July, (knowing that it was useless) and because they were advised to get huge supplies of this drug (Table 3), which promptly took place (European Commission) (K).
Because a worldwide race for vaccines began, unsafe both for the abbreviated test procedure due to the Covid emergency, but also for the strong economic interests (the over 160 centers in the world have been sponsored on average with 200 Million Euro). There is also hardly any state control of the trials. The sponsor (i.e. who pays for the trials with a high compensation to the hospitals) and the ethical commission are responsible for controlling the correct conduct of the trial itself (the dream of every student: I write the assignment, I mark it and give it a grade). Vaccination during an ongoing epidemic can also trigger serious side effects like the narcolepsy during the vaccination against swine ‘flu in 2009.
In this epidemic too the political reaction proved completely exaggerated. The EU (to name some countries) spent about 1.3 billion in England and over 700 million in France for a vaccine for a ‘flu which had caused only 2,900 deaths in Europe compared to the European average of 40,000 to 220,000 a year from common ‘flu (EC debate 7/3/2011) (L). In 2009 Transparency International (The Global Coalition against Corruption) had already criticized the financing of the European Medicines Agency (EMA) for two thirds of the Pharmaceutical Industry (M). The European Court of Auditors later confirmed this conflict of interest (Press release ECA/12/39 on 11/10/2012) (N).Whoever performs vaccination during an ongoing epidemic commits a graveerror
Because the “VirologicalScience” does not admit to having wrongly assessed the means of transmission of the Coronavirus (O). It is in the same situation as Gottlob Frege (1902), who in the end discovered important errors in his research defining the bases of mathematics (note 3).
Because there is a relentlessness towards children, our future, considering them global super-spreaders.
TRAUMATIZING CHILDREN CONSTITUTES A CRIME AGAINST “HUMANITY”
The answer my friends, is blowing in the wind, the answer is blowing in the wind.
Appendix
Table 1) – Percentage variation in deaths in 2020 compared to the 2015-2019 average, by region, distribution and month.
Report ISTAT, National Institute of Statistics, 22/10/2020
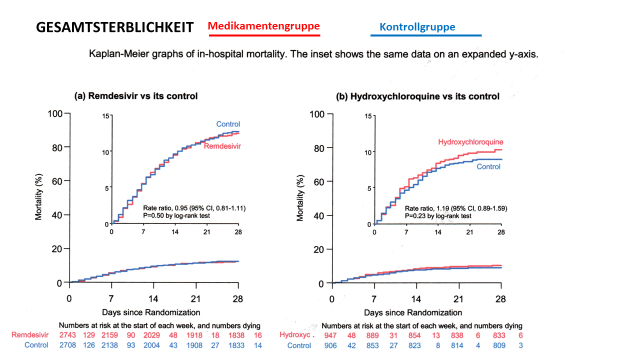
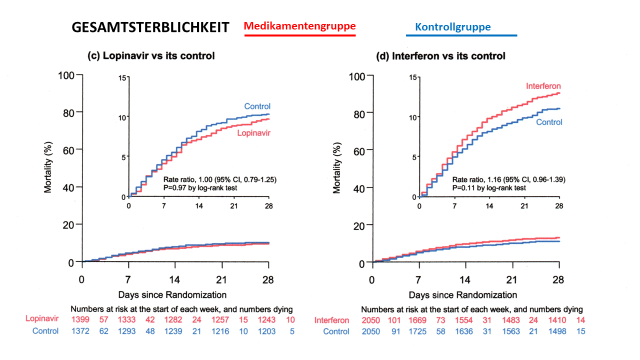
Table 2)
Statistical elaboration: Kaplan Meier 28 day risks (mortality), available monthly from April on the WHO site. The monthly results have clearly shown the inefficacy of the antiviral drugs involved, hence the study should have been interrupted much sooner. Each month of delay causes unnecessary deaths.
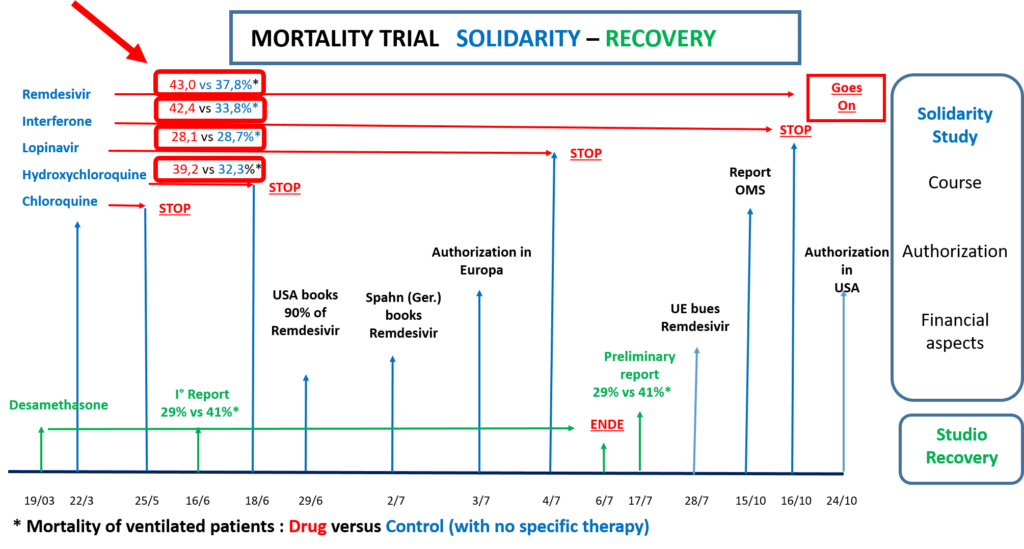
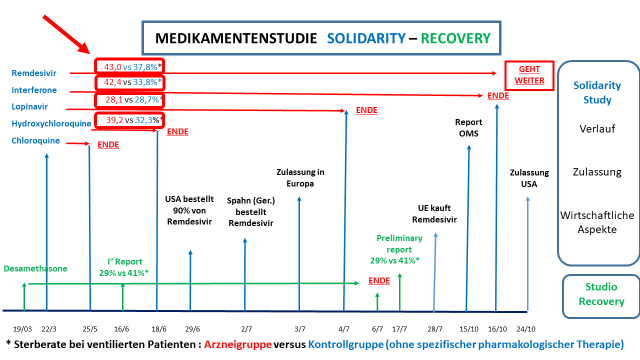
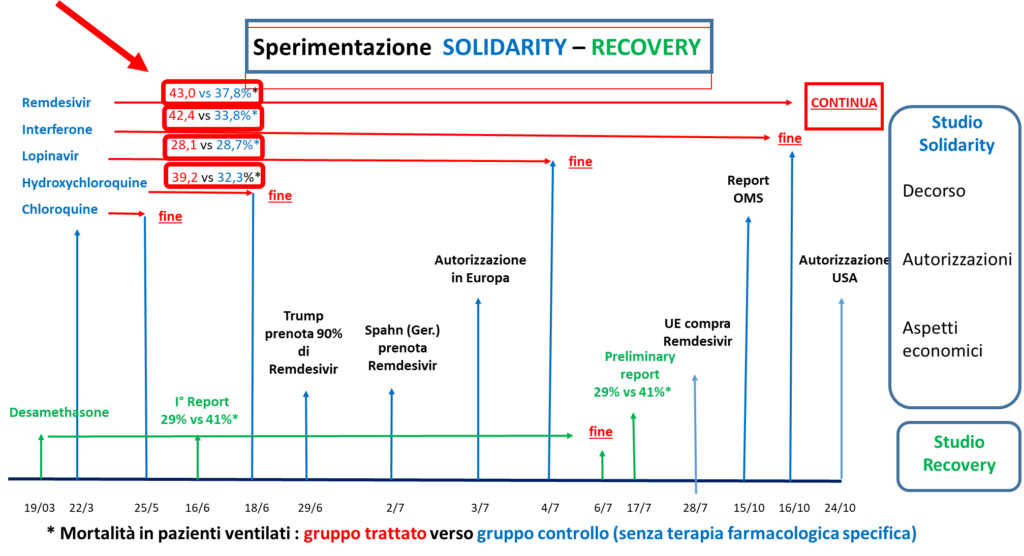
Timeline of the experiments (Mortality PV* = Ventilated Patients, control** = with no specific therapy)
19/03 Recovery trial begins
22/3 Solidarity (S) trial begins monthly report of results
15/10 WHO Report Mortality PV* Remdesivir 43.0%, control** 37.8%
24/10 USA authorizes the use of Remdesivir
Note 1) “National Health Institute, Report n.49/2020, 8/6/2020: “COVID-19: Interim Report on the definition, certification and classification of the causes of death”
According to this report the patients included in the 33.000 until 7/6/20 are composed as follows:
Suspected case (without laboratory investigation: Author’s note)
Someone with acute respiratory infection and with no other etiology, which completely explains the clinical presentation and with a travel or residence history with transmission of the virus.
Someone with any acute respiratory Infection who has been in contact with a probable or confirmed case of Covid.
Probable case: suspected case whose SARS-CoV-2 test result is doubtful or inconclusive (i.e. despite negative test the diagnosis is confirmed: Author’s note)
Confirmed case. Case with laboratory confirmation independently of signs and clinical symptoms.
Note 2) “National Institute of Statistics” ISTAT Report from 16/7/20: “Impact of the Covid-19 epidemic on Mortality: Causes of death of positive deceased from SARS-CoV-2”
The report includes 4,942 statements of death submitted to the National Institute of Health with confirmed SARS-CoV infection. This constitutes only 15.6% of the reported cases until 25/5/20 out of a total of 31.573 deaths. Therefore the remaining cases are suspected or probable cases (i.e.with no laboratory diagnosis).
The statistical elaboration of this small group of patients has emphasised that: “Covid-19 is the directly responsibile cause of death in 89% of deaths of people positive to SARS-CoV-2”, a statement which is repeated daily like a prayer wheel.
Definition of directly responsibile for death: death is caused directly by Covid-19, when death would not have been verified, if the SARS-Cov-2 infection had not intervened (although often overlapping other pre-existing illnesses and their complications).
Note 3) The virological community should publicly release the same declaration as Frege on 16/6/1902 (modified by vaso di pandora): “Hardly anything more unwelcome can befall a scientific writer (virological community) than that one of the foundations of his edifice be shaken after the work (program for the “fight” against the pandemic) is finished. This is the position into which I was put (still Frege) by a letter from Mr Betrand Russell (Wegener der Weltbildzertruemmerer), as the printing of this volume (Public Measures against the Pandemic) was nearing completion.
Ministero della Salute Italiano: Covid-19: Situazione in Italia al 4/11/2020. http://www.salute.gov.it/portale/nuovocoronavirus/dettaglioContenutiNuovoCoronavirus.jsp?area=nuovoCoronavirus&id
D) Istituto Superiore della Sanità (ISS): COVID-19: rapporto ad interim su definizione, certificazione e classificazione delle cause di morte, n.49/2020. 8/6/20
E) Istituto di Statistica Italiana: Impatto dell’epidemia COVID-19 sulla mortalità: cause di morte nei deceduti positivi a SARS-COV-2, https://www.istat.it/it/archivio/245573
CETERO CENSEO, CARTAGINEM ESSE DELANDAM, so endete Cato Major jede seiner Reden im Senat,
und in diesem Sinne: Ceterum censeo, dass die derzeitige Lage in keinster Weise medizinischer Natur ist, sondern nur politischer und oekonomischer. Das oeffentliche Wohl und die Gesundheit hat damit nichts zu tun, der gemeine Buerger ist nur Kannonenfutter.
Weswegen erfolgt taeglich oeffentliche organisierte Fehlinformation der Bevoelkerung bezueglich Mortalitaet, Laetalitaet, Erkrankten, Reproduktionszahl, Toten, Neuinfektionen, Reinfektionen, und Asymptomatischen. Letztere werden mittlerweile mit allen dem Staat verfuegbaren Mitteln verfolgt, als waeren sie Verbrecher, obwohl alle Statistiken aufzeigen, dass keinerlei Zusammenhang zwischen neuen Positiven und Todesfaellen besteht (A).
Weswegen werden jeden Tag neue Schreckensnachrichten hinsichtlich der Coronapandemie verbreitet, obwohl in diesem Jahr (hier Italien als Beispiel, in Deutschland sind diesbezuegliche Daten allgemein nicht abrufbar) kein statistisch signifikanter Anstieg der Sterblichkeit hinsichtlich des Zeitraumes 2015-19 zu verzeichnen ist. Im Zeitraum Mai – August 2020 wurde eine Verringerung der Sterblichkeit in Italien bezueglich 2015-2019 um 1,6% verzeichnet (Report ISTAT. Istituto Nazionale di Statistica, 22/10/2020, (Tabella 1)(B).
Weswegen sehen die “medialen “ Statistiken einen betraechtlichen Anstieg der „Coronatoten“ vor mit duesteren Zukunftsprognosen (bald mehr als 1000 Tode pro Tag), obwohl die Coronafallsterblichkeit nur 0.2% betraegt (World Health Organisation, 14/10/2020)(C). Liegt dies eventuell auch daran, dass auch Patienten mit reiner Verdachtsdiagnose (aufgrund medizinischer oder epidemilogischer Einschaetzung), ohne labortechnischem Nachweis mit eingeschlossen werden (Fussnote 1, Report des Istituto Superiore della Sanità (ISS), n.49/2020, 8/6/2020)(D)? Oder koennte dies durch die statistische Aufarbeitungen von nur begrenzten Patientenkollektiven (4942 von insgesamt 31.573 Coronatoten) oder auch durch die unzutreffende Definitionen verursacht werden. Unter „Direkt verantwortlich fuer den Todesfall“ wird definiert, dass der Tod nicht eingetreten waere, wenn die SARS-CoV-2 Infektion nicht erfolgt waere, obwohl haeufig Vorerkrankungen oder ihre Komplikationen gleichzeitig vorhanden sind“ (Report des „Istituto Nazionale di Statistica“ (ISTAT) del 16/7/2020:.”Impatto dell’Epidemia Covid-19 sulla Mortalità: Cause di morte dei deceduti positivi a SARS-Cov-2”, Fussnote 2)(E)?
Weswegen sind zur Zeit in ganz Europa die Krankenhaeuser aufgrund Coronapatienten fast ausgelastet, obwohl die Sterblichkeit zur Zeit nur ungefaehr 10-20% derer des Fruehjahres betraegt? Ausserdem wurden mittlerweile die Kapazitaeten von Krankenhausplaetzen fuer Coronapatienten erhoeht. Dient dies dazu, das Defizit der Krankenhaeuser aufgrund der dramatische Unterbelegung infolge der Coronaepidemie auszugleichen (Defizit in den ersten 4 Monaten in Italien von 3.5 Miliarden Report ALTEMS Alta Scuola di Economia e Management dei Sistemi Sanitari) (F). So kann das jaehrliche Budget erreicht werden, um nicht insolvent zu werden („Coronakrise rettet die Kliniken – aber die Pleitegefahr bleibt hoch Das Handelsblatt, Germania) (G). In Deutschland zahlt mittlerweile der Staat fuer jedes unbelegte Krankenhausbett 700 Euro taeglich „in Erwartung der zweiten Coronawelle“. All dies, da direkte Subventionen in der UE nicht mehr erlaubt sind. Kann jemand seinen finanziellen Verpflichtungen nicht nachkommen, muss er Konkurs anmelden, undenkbar fuer das Gesundheitssystem, ein Supergau.
Weswegen wurden im Maerz klinische Studien auf weltweiter Ebene bezueglich der Wirksamkeit antiviraler Medikamenten wie Remdesivi (Solidarity etc.) autorisiert, bei der die Kontrollgruppe keiner spezifischen pharmakologischen Therapie unterzogen wurde, die jedoch das Kortison haette sein muessen. Diese Studien hatten weltweit unzaehlige aehnliche Studien mit denselben unnuetzen Medikamenten als Folge, mit denselben enttaeuschenden Ergebnissen
Weswegen fuehrte man diese Studien fuer viele Monate weiter, obwohl bereits nach einem Monat deutlich war (statistische Auswertung: Kaplan Meier 28 Day Mortality, Tabelle 2) (H), dass die Medikamente nicht nur voellig unwirksam waren, sondern sogar eine hoehere Sterberate als bei der Kontrollgruppe ohne jeglicher speziefischer Therapie verursachten. Die Sterblichkeit von ventilierten Patienten lag bei 41% (Trial Solidarity), waehren die von ventilierten Patienten unter Kortisongabe (Trail Recovery) bei 29% lag (I).Diese pharmakologischen Studien haben somit den Tod von vielen Menschen unter dem Vorwand der wissenschaftlichen Forschung verursacht, und all dies ohne grossteils eine Pazienteneinwilligung fuer diese Studien einzuholen. Die Gesetzgebung in Europa befreite die „Sponsoren“ aufgrund des Covidnotfalles davon, unter schwerwiegenster Verletzung der Rechte der Erkrankten (European Medicines Agency et al.) (J). Kein Patient/Angehoeriger haette jemals eine Einwilligung unterschrieben mit der Erklaerung, dass die Haelfte der Studienteilnehmer ohne spezifischer medizinischer Therapie gelassen wurde, sondern nur mit einem Placebo.
Weswegen wurden den Regierungen empfohlen, Remdesivir am 3. Juli in Europa zuzulassen, obwohl seit Monaten deren Unwirksamkeit nachgewiesen war, und weswegen wurden Vorraete dieses unnuetzen Medikamentes in grossen Mengen von Europa (European Commission) (K) erworben (Tabelle 3).
Weswegen wurde das Rennen um die Impfung auf der ganzen Welt eroeffnet, fuer eine Impfung die unsicher ist, sowohl aufgrund der abgekuerzten Versuchsdauer wegen der Notfallsituation Coronavirus, als auch wegen immensen finanziellen Interessen (die mehr als 160 Zentren, sind im Durchschnitt mit 200 Millionen Euro gesponsort). Hier fehlt fast vollstaendig eine staatliche Kontrolle der Studienablaeufe. Der Sponsor (derjenige der die Krankenhaeuser mit grosser finanzieller Zuwendung die Studien durchfuehren laest) ist selbst, mit der Ethikkommission, dafuer verantwortlich, die eigenen Studienvorgaben zu erfuellen. (ein Traum eines jeden Schuelers: Ich schreibe meine Schulaufgabe, ich korrigiere sie selbst und benote mich dann selbst). Ausserdem fuehrt eine Impfung waehrend einer Epidemie zu schweren Zwischenfaellen wie die Narkolepsie aufgrund der Schweinegrippeimpfung 2009. Auch bei dieser Epidemie war die politische Antwort vollkommen uebertrieben. Es wurden von der Europaeischen Union (um nur ein paar Laender zu nennen) ungefaehr 1.3 Miliarden in England, mehr als 700 Millionen in Frankreich fuer diese Impfung ausgegeben, obwohl nur 2900 Todesfaellen in Europa am Ende zu registrieren war. Im Vergleich versterben an der saisonalen Grippe in Europa jaehrlich 40.000-220.000 Menschen (siehe Plenardebatte 7/3/2011 der Europaeischen Union) (L). Trasparency International (The Global Coalition against Corruption) hatte bereits 2009 die Finanzierung der Europaeischen Arzneimittelargentur (EMA) zu fast zwei Dritteln durch die pharmazeutische Industrie kritisiert (M). Der Europaeische Rechnungshof hat diese Interessenkonflikte oeffentlich bestaetigt (Pressemitteilung ECA/12/39 vom 11/10/2012) (N).Wer eine Impfung waehrend einer laufenden Epidemie durchfuehrt, beginnt einen medizinischen Fehler.
Weswegen gibt die “Virologische Wissenschaft” nicht zu, dass sie den Uebertragungsweg des Coronavirus falsch beurteilt hat (“Seit man begonnen hat, einfachste Behauptungen zu beweisen, erweisen sich viele als falsch: Zitat Russel Bertrand). Sie ist in der gleichen Lage von Gottlob Frege (O), der beim Versuch, die Basis der Mathematik zu definieren, auf eigene fundamentale Fehler gestossen war (Fussnote 3)
Weswegen werden die Kinder, ins Visier genommen, unsere Zukunft, als waeren sie diejenigen, die die Welt infizierten.
KINDER ZU TRAUMATISIEREN IST EIN VERBRECHEN GEGEN DIE MENSCHLICHKEIT.
The answer my friends, is blowing in the wind, the answer is blowing in the wind.
Tabelle 1)
Tabelle 2)
Statistik: Kaplan Meier 28 day mortality (seit April monatlich abrufbar ueber die Home page WHO).Die Ergebnisse haben monatlich die Unwirksamkeit der angewandten Arzneimittel dargelegt. Die Studie haette baldmoeglichst abgebrochen werden muessen, um weiter Todesfaelle“ im Namen der wissenschaftlichen Forschung“ zu vermeiden.
Tabelle 3)
Chronologie der klinischen Studien: Versuchsgruppe, Kontrollgruppe (ohne spezifischer pharmakologischer Therapie), Sterblichkeit von ventilierten Patienten in %
19/03 Anfang des Trial Recovery: ( Kortison)
22/3 Anfang des Trial Solidarity: (Chloroquine, Hydrochloroquine, Lopinavir, Interferone, Remdesivir)
25/5 Ende Chloroquine im Trial Solidarity
16/6 I° Report Recovery
Kortisone: 29%, Kontrollgruppe 41%
18/6 Ende Hydroxychloroquine im Trial Solidarity:
H.chloroquine 39.2%, Kontrollguppe. 32.3%
29/6 USA bestellen 90% von Remdesivir vor
2/7 Deutschland bestellt Remdesivir vor
3/7 UE laesst Remdesivir in Europa zu
4/7 Ende Lopinavir im Trial Solidarity
Lopinavir 28.1%, Kontrollgruppe 28.7%
6/7 Ende Trial Recovery
17/7 Report Trial Recovery
Cortisone 29%, Kontrollgruppe 41%
28/7 UE erwirbt Remdesivir
15/10 Report WHO
Remdesivir 43.0%, Kontrollgruppe 37.8%
16/10 Ende Interferone im Trial Solidarity
Interferone 42.4%, Kontrollgruppe 33.8%
24/10 USA laesst Remdesivir zu
Fussnote 1)
Report des “Istituto Superiore della Sanità”, n.49/2020, 8/6/2020: “COVID-19: rapporto ad interim su definizione, certificazione e classificazione delle cause di morte”
Gemaess diesem Report setzt sich das Patientengut der statistischen Covid-2 Erfassung in Italien (mehr als 33.000 Todesfaelle bis zum 7/6/20), wie folgt zusammen:
1) Verdachtsfaelle (ohne Labornachweis, Note des Autors)
a) Patienten mit akuter respiratorischer Infektion, keiner anderen Aethiologie, Reise oder Wohnort in einem Gebiet mit lokaler Uebertragungsgefahr.
b) Patienten mit jeglichem akutem respiratorischem Infekt, die in den vorhergegangenen 15 Tagen mit einem moeglichem oder bestaetigten Coronaerkrankten in Kontakt gekommen sind.
c) Patienten mit akutem respiratorischem Infekt, der eine Krankenhauseinweisung erfordert (keine anderen Aethiologie).
(Dies ohne Labornachweis)
2) Wahrscheinliche Faelle: Verdachtsfaelle mit fraglichen oder unschluessige Ergebnissen des Labortest SARS-Cov-2
3) Sichere Faelle: Personen mit positivem Labortest unabhaengig von klinischen Krankheitszeichen oder Symptomen.
Fussnote 2)
Report des „Istituto Nazionale di Statistica“ (ISTAT) del 16/7/2020:.”Impatto dell’Epidemia Covid-19 sulla Mortalità: Cause di morte dei deceduti positivi a SARS-Cov-2”
Der Report umfasst 4942 Todesmeldungen von Patienten mit nachgewiesener Covid-19 Infektion, die der Staatlichen Institution „Istitut Superiore della Sanità“ zugesandt wurden. Sie stellen nur 15.6% der Gesamttodesfaelle (31.573 zum 25/5/2020) dar. Somit sind wahrscheinlich der Rest (26.631) Verdachtsfaelle oder wahrscheinliche Faelle (alle also ohne positivem Labortest).
Die Auswertung dieses kleinen Patientenkollektives ergab folgendes Ergebnis:
COVID-19 ist im 89% der Todesfaelle direkt fuer den Tod von SARS-CoV-2 positiven Patienten verantwortlich.
Unter dem Begriff: direkt verantwortlich versteht man, dass der Tod nicht erfolgt waere, wenn die SARS-CoV-2 Infektion nicht eingetreten waere, obwohl haeufig Vorerkrankungen oder ihre Komplikationen gleichzeitig vorhanden sind.
Fussnote 3)
Die Virologische Gesellschaft muesste mehr oder weniger dieselbe oeffentliche Erklaerung abgeben wie Frege am 16/06/1902 (modifiziert nach Vaso di Pandora): „Einem wissenschaftlichen Schriftsteller (der virologischen Gemeinschaft) kann kaum etwas Unerwünschteres begegnen, als daß ihm nach Vollendung einer Arbeit (Progamm fuer die Bekaempfung der Pandemie), eine der Grundlagen seines Baues erschüttert wird. — In diese Lage wurde ich (Frege) durch einen Brief des Herrn Bertrand Russell (Wegener, der Weltbildzertruemmerer) versetzt, als der Druck dieses Bandes (Oeffentliche Massnahmen zur Bekaempfung der Pandemie) sich seinem Ende näherte”.
Ceterum censeo, Cartaginem esse delendam
Ossia :
La costruzione delle bugie crollerà
CETERUM CENSEO, CARTAGINEM ESSE DELENDAM, così finiva Catone, il Censore, ogni suo intervento al senato.
In tale senso: Ceterum Censeo, che la situazione non è di natura medica ma di natura politica/economica, il bene e la salute pubblica non c’entra niente, le persone comuni non sono altro che carne da cannone:
Curva -Giallo : attualmente positivi, Verde: guariti, Grigio: decessi
Perché avviene giornalmente una disinformazione organizzata della popolazione riguardante mortalità, letalità, indice di contagiosità, deceduti, infetti nuovi, reinfezione, asintomatici, portatori sani, positivi. Quest’ultimi vengono inseguiti con tutti i mezzi a disposizione dello stato, come se fossero dei delinquenti. Ma questa caccia non ha senso, essendo l’indice di contagiosità completamente scollegato dalla mortalità, come evidenziato dalla statistica emessa dal governo italiano il 4/11/20 (A).
Perché vengono diffuse ogni giorno notizie disastrose per quanto riguarda la pandemia, nonostante che in questo anno (Italia come esempio, in Germania non sono disponibili i dati a tale proposito) non c’è stato un aumento statisticamente significativo della mortalità rispetto al periodo 2015-2019. Nel periodo maggio-agosto ci fu addirittura una riduzione della mortalità rispetto ai cinque anni precedenti del 1.6% (Report ISTAT, Istituto Nazionale di Statistica, 22/10/2020 (Tabella 1)(B).
Perché le statistiche diffuse dalle media prevedono un aumento considerevole dei decessi da coronavirus con previsioni angoscianti per il futuro, (“fra poco più di 1000 morti al giorno”), nonostante la letalità da Coronavirus viene stimato del 0.14% contro il 0.10 della influenza comune (WHO 14/10/20)(C). Questo forse perché pazienti anche senza conferma di laboratorio, vengono inclusi nella mortalità con la sola diagnosi di sospetto (a causa di valutazione medica o epidemilogica) (Rapporto del Istituto Superiore della Sanità (ISS), n.49/2020,8/6/20, nota 1)(D), oppure perché la elaborazione statistica fu eseguita su gruppi limitati di pazienti (4942 di 31.573 morti per Coronavirus al 25/05/2020), oppure perché sono stati utilizzati termini di definizioni inadatte. Sotto il termine “direttamente responsabile per il decesso”, si intende, che il decesso non si sarebbe verificato se l’infezione da SARS-CoV-2 non fosse intervenuta, seppure spesso sovrapposto ad altre malattie preesistenti, e dalle sue complicanze (Report del “Istituto Nazionale di Statistica” ISTAT) del16/7/2020: Impatto dell’epidemia Covid-19 sulla mortalità: Cause di morte dei positivi a SARS-CoV-2, nota 2)(E).
Attualmente quasi tutti i ospedali in quasi tutto l’Europa sono pressoché pieni di pazienti di Coronavirus, nonostante la mortalità attuale è molto inferiore rispetto alla primavera. Inoltre nel frattempo fu aumentata la capacità dei letti ospedalieri per pazienti da Coronavirus,. Potrebbe servire questo, per recuperare il deficit dei ospedali causato dalla drammatica riduzione dei accessi ai ospedali a causa della pandemia (il deficit nei primi 4 mesi in Italia è di 3.5: Report ALTEMS Alta Scuola di Economia e Management dei sistemi Sanitari) (F). In tale maniera si può raggiungere il Budget, per non rimanere insolvente (“Coronavirus rettet die Kliniken, aber die Pleitegefahr bleibt hoch” = la crisi da coronavirus salva gli ospedali, ma il rischio di fallimento rimane alto. Das Handelsblatt ) (G). In Germania lo stato paga ai ospedali circa 700 euro per ogni letto non occupato con la motivazione, di tenerlo libero per l’attesa della eventuale seconda onda della pandemia. Tutto questo perché sovvenzioni diretti a livello della Communita europea non sono più permessi. Se qualcuno non può rispettare i suoi obblighi finanziari, deve dichiarare insolvenza, un disastro per la sanità pubblica.
Perché venivano autorizzate a marzo sperimentazioni a largo spettro a livello mondiale di farmaci antivirali quali Remdesivir (Solodarity ecc.) con il gruppo di controllo, che non otteneva nessuna terapia farmacologica specifica, che invece doveva essere il cortisone. Nella loro scia sono state sperimentate quasi ovunque le stesse medicine inutili.
Perché si insisteva nella sperimentazione per molti mesi per appurare che la terapia aveva alcun beneficio, il che era già evidente dopo un mese (elaborazione statistica tramite metodo Kaplan Meier 28 Day Mortality, Tabella 2) (H). Anzi la mortalità era addirittura superiore al gruppo di controllo. La mortalità in questi studi per pazienti ventilati era del 41% (studio Solidarity), mentre quella con la terapia con cortisone era del 29% (Studio Recovery) (I).Tutte queste sperimentazioni farmaceutiche inutili hanno causato la morte di migliaia di persone con il pretesto della ricerca scientifica. E tutto questo in linea di massima senza aver chiesto ed ottenuto il consenso informato da parte dei pazienti/parenti, perché un a disposizione legge in Europa esonerava per l’emergenza Covid lo sperimentatore da questo obbligo (European Medicines Agency ecc.) (J), ledendo in maniera grave i diritti costituzionali fondamentali di ogni cittadino. Nessuno paziente oppure parente avrebbe firmato un consenso informato contenente l’affermazione, che la metà dei malati venivano lasciati senza terapia di riferimento ma solo con il placebo.
Perché fu consigliato ai governi europei di autorizzare l’utilizzo del Remdesivir il 3 Luglio, (sapendo che era inutile e perché fu consigliato a loro di fare approvvigionamenti ingenti di tale farmaco (Tabella 3),.come prontamente avvenuto (European Commission) (K).
Perché fu iniziata una corsa ai vaccini in tutto il mondo, insicuro sia per la procedura di sperimentazione abbreviata a causa della emergenza Covid, ma pure per i forti interessi economici (i oltre 160 centri nel mondo sono sponsorizzati mediamente con 200 Milione di Euro). Inoltre manca pressoché completamente un controllo statale dei studi. Lo sponsor (cioè chi paga la sperimentazione con un forte compenso ai ospedali) e la commissione etica sono i responsabili per controllare il corretto svolgimento della sperimentazione stessa (il sogno di ognun studente: io scrivo il compito, il lo correggo ed io do il voto). Inoltre la vaccinazione durante una epidemia in corso può comportare dei seri effetti collaterali come la narcolessia durante la vaccinazione contro l’influenza suina del 2009. Anche in questa epidemia la reazione politica si era dimostrato completamento esagerata. Sono stati spesi dall’Unione Europea (per nominare alcuni paesi) circa 1.3 miliardi in Inghilterra e oltre 700 milioni in Francia per il vaccino per una influenza, che aveva causato in Europa solo 2900 decessi rispetto alla media in Europa della influenza comune di 40.000 a 220.000 l’anno (dibattito Comunione Europea del 7/3/2011) (L). Trasparency International (The Global Coalition against Corruption) aveva già nel 2009 criticato il finanziamento della Agenzia Europea del Farmaco (EMA) per i due terzi dalla Industria Farmaceutica (M). In seguito la Corte dei Conti Europea ha confermato questo conflitto d’interesse (Comunicazione stampa ECA/12/39 del 11/10/2012) (N).Chi effettua una vaccinazione durante una epidemia in corso commette un grave errore
Perché la “Scienza Virologica” non ammette, di aver valutato in maniera sbagliata la via di trasmissione del Coronavirus (O). Essa trova nella stessa situazione come Gottlob Frege (1902), che nella sua ricerca, di definire le basi della matematica, alla fine ha riscontrato dei errori importanti (nota 3).
Perché c’è un accanimento contro i bambini, il nostro futuro, considerandoli untori del mondo (lavori dei bambini).
TRAUMATIZZARE I BAMBINI COSTITUISCE UN CRIMINE CONTRO L‘UMANITA’
The answer my friends, is blowing in the wind, the answer is blowing in the wind.
Appendice
Tabella 1)
Report ISTAT, Istituto Nazionale di Statistica, 22/10/2020
Tabella 2)
Elaborazione statistica: Kaplan Meier 28 day risks (mortality), da aprile mensilmente consultabile presso il sito OMS. I risultati mensilmente hanno chiaramente dimostrato l’inefficacia dei farmaci antivirali impegnati, per cui lo studio doveva essere interrotto molto prima. Ogni mese di ritardo è causa di decessi evitabili.
Tabella 3)
Cronologia delle sperimentazioni (Mortalità PV* = Pazienti Ventilati, controllo** = senza terapia specifica)
Cronologia delle sperimentazioni: Gruppo trattato, gruppo controllo (senza terapia farmacologica specifica), mortalità di pazienti ventilati in %
19/03 Inizio trial Recovery Cortisone
22/3 Inizio trial Solidarity (S) Chloroquine, Hydroxychloroquine, Lopinavir, Interferone, Remdesivir
25/5 Chloroquine esce da Solidarity
16/6 I° Report Recovery Cortisone: 29%, controllo : 41%
18/6 Hydroxychloroquine esce da Solidarity
H.chloroquine : 39.2%, controllo : 32.3%
29/6 USA prenotano 90% delle risorse Remdesivir
2/7 Germania prenota Remdesivir
3/7 Autorizzazione Unione Europea (UE)
4/7 Lopinavir esce da Solidarity
Lopinavir : 28.1%, controllo 28.7%
6/7 Fine trial Recovery
17/7 Report trial Recovery Cortisone : 29%, controllo : 41%
28/7 UE compra Remdesivir
15/10 Report WHO Remdesivir : 43.0%, controllo : 37.8%
16/10 Interferone esce da Solidarity
Interferone : 42.4%, controllo : 33.8%
24/10 Autorizzazione USA
Nota 1) Report dell’”Istituto Superiore della Sanità, n.49/2020, 8/6/2020: “COVID-19: Rapporto ad interim su definizione, certificazione e classificazione delle cause di morte”
Secondo questo rapporto i pazienti inclusi nei 33.000 fino al 7/6/20 si compongono come segue:
Caso sospetto (senza indagine di laboratorio: Nota dell’autore) :
Persona con infezione respiratoria acuta e senza un’altra eziologia, che spieghi completamente la presentazione clinica e con storia di viaggi o residenza con trasmissione del virus.
Persona con qualsiasi infezione respiratoria acuta che è stato in contatto con caso probabile o confermato Covid.
Caso probabile: caso sospetto il cui risultato al test per SARS-CoV-2 è dubbio o inconcludente (cioè nonostante test negativo viene confermato la diagnosi: Nota dell’autore)
Caso confermato. Caso con conferma di laboratorio indipendentemente dai segni e dai sintomi clinici.
Nota 2) Report dell’”Istituto Nazionale di Statistica” ISTAT del 16/7/20: “Impatto dell’epidemia Covid-19 sulla Mortalità: Causa di morte dei deceduti positivi al SARS-CoV-2”
Il rapporto include 4942 schede di morte pervenute all’ Istituto superiore della Sanità con infezione da SARS-CoV confermati. Questo costituisce solo il 15.6% dei casi segnalati fino al 25/5/20 su un totale di 31.573 deceduti. Il rimanenti casi sono allora casi sospetti o probabili (cioè senza diagnosi di laboratorio.)
La elaborazione statistica di questo esiguo gruppo di paziente ha evidenziato che: “Covid-19 è la causa direttamente responsabile della morte nell’89% dei decessi di persone positive al SARS-CoV-2”, una affermazione, che viene giornalmente ripetuta come una ruota della preghiera.
Definizione direttamente responsabile per la morte: la morte è causata direttamente da Covid-19, quando il decesso non si sarebbe verificato, se l’infezione da SARS-Cov-2 non fosse intervenuta (seppure spesso sovrapposto ad altre malattie preesistenti e delle sue complicanze).
Nota 3) La comunità virologica dovrebbe rilasciare pubblicamente la stessa dichiarazione come Frege il 16/6/1902 (modificato da vaso di pandora): Ad un autore scientifico (comunità virologica) difficilmente puo accadere una cosa piu indesiderata dopo la il completamento della sua opera (programma per la “lotta” contro la pandemia), che una base della sua costruzione viene scosso. In questa situazione mi sono trovato (sempre Frege) a causa della lettera del Sig. Bertrand Russell (Wegener der Weltbildzertruemmerer), quando la stampa del mio libro (Misure Pubblichecontro la Pandemia) giungeva alla fine.
D) Istituto Superiore della Sanità (ISS): COVID-19: rapporto ad interim su definizione, certificazione e classificazione delle cause di morte, n.49/2020. 8/6/20
E) Istituto di Statistica Italiana: Impatto dell’epidemia COVID-19 sulla mortalità: cause di morte nei deceduti positivi a SARS-COV-2, https://www.istat.it/it/archivio/245573